National Early Season Flu Vaccination Coverage, United States, November 2015
Influenza (flu) is a contagious respiratory illness that can cause mild to severe illness. Serious outcomes of flu infection can result in hospitalization and sometimes even death.
- Anyone can get sick from the flu.
- Some people, such as older people, young children, and people with certain health conditions are at higher risk for flu-related complications, such as pneumonia.
Flu vaccination is the best way to prevent the flu and potentially serious flu-related complications (1, 2). The Centers for Disease Control and Prevention (CDC) recommends that everyone 6 months and older get a flu vaccination each flu season (3).
This report summarizes data from the National Immunization Survey-Flu (NIS-Flu) for children 6 months through 17 years and the National Internet Flu Survey (NIFS) for adults 18 years or older. NIS-Flu data were collected by telephone surveys of parents conducted during October 1–November 14, 2015, while the NIFS data were collected through an Internet panel survey conducted during October 29–November 11, 2015. This report provides early flu season estimates of how many people (children and adults) in the United States had received a flu vaccination. Final 2015–16 flu season vaccination coverage estimates will be available after the end of the season.
Key Findings
- Fewer than half of children and adults were vaccinated by early November 2015 (early flu season):
- 39.7% of all persons 6 months and older
- 39.2% of children 6 months through 17 years
- 39.9% of adults 18 years and older
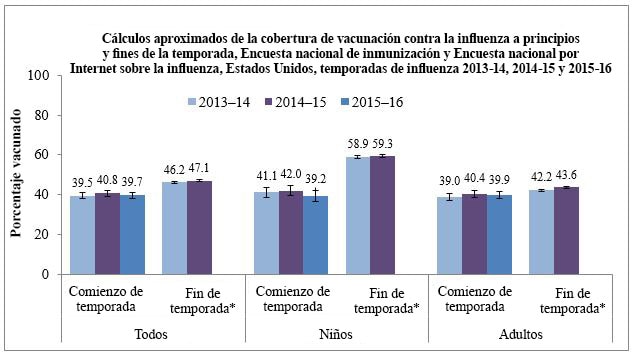
- Early 2015–16 flu season vaccination coverage was similar to coverage at the same time last flu season for children, adults, and all persons 6 months and older.
- Among children, early season flu vaccination coverage among non-Hispanic whites was 5.0 percentage points lower compared to the same time last season.
- Non-Hispanic black children and children of non-Hispanic other or multiple races had higher flu vaccination coverage than non-Hispanic white children. Early season flu vaccination coverage among children was similar across all other racial/ethnic groups.
- Non-Hispanic black adults had lower flu vaccination coverage than non-Hispanic white adults. Early season flu vaccination coverage among adults was similar across other racial/ethnic groups.
- Among both adults and children, the most common places reported for receiving flu vaccination were medical locations (children: 86.4%, adults: 47.9%). Retail settings (24.8%) and workplaces (18.1%) were other important venues for adults.
Conclusions/Recommendations:
- As of early November 2015, only 2 out of every 5 persons 6 months and older in the United States had received a flu vaccine, leaving most persons without the protection afforded by flu vaccination.
- Individuals not yet vaccinated this season should get a flu vaccination as soon as possible.
- A provider recommendation to get a flu vaccination is an important factor in a patient’s decision to get vaccinated. All providers should routinely assess the flu vaccination status of their patients at every clinical encounter, strongly recommend flu vaccination, and provide flu vaccination or, if they do not stock flu vaccine, refer the patient to a vaccine provider for flu vaccination (4).
- Vaccination providers and immunization programs should work to increase community demand for vaccination and expand access to vaccination services.
- Worksites can collaborate with vaccination providers and immunization programs to promote flu vaccination and even offer vaccination at work.
- Vaccination providers should have systems in place to routinely assess patients for vaccination status and ensure that unvaccinated patients receive a strong recommendation for vaccination.
- Provider reminders and standing orders are systems that can prove useful in healthcare settings.
Who Was Vaccinated?
Flu Vaccination Coverage by Age Group
- Flu vaccination coverage early in the 2015–16 season was 39.7%, similar to coverage estimates for the same time last flu season (40.8%) (Table 1).
|
November 2014 |
November 2015 |
|
|---|---|---|
| Overall (≥ 6 months) |
40.8 ± 1.5 |
39.7 ± 1.6 |
| Children (6 months–17 years) |
42.0 ± 2.5 |
39.2 ± 2.7 |
| Adults (≥ 18 years) |
40.4 ± 1.8 |
39.9 ± 1.9 |
- Among children 6 months through 17 years, early season flu vaccination coverage with one or more doses was 39.2% as of early November, similar to coverage estimates from the same time last flu season (Table 2).
- All child age groups had similar coverage compared to the same time last season.
- Flu vaccination coverage among children decreased as age increased.
- Flu vaccination coverage was highest among children 6 months–4 years (51.7%) and lowest among children 13–17 years (26.6%).
|
Age Group |
November 2014 |
November 2015 |
|---|---|---|
| All children (6 months-17 years) |
42.0 ± 2.5 |
39.2 ± 2.7 |
| 6 months-4 years |
49.7 ± 5.2 |
51.7 ± 6.1 |
| 5-12 years |
44.6 ± 3.8 |
40.7 ± 3.6 |
| 13-17 years |
31.8 ± 3.9 |
26.6 ± 4.5 |
- Among adults 18 years and older, early season flu vaccination coverage as of early November was 39.9%, similar to the same time last flu season (Table 3).
- All adult age groups had similar coverage compared to the same time last season.
- Flu vaccination coverage among adults increased as age increased.
- Vaccination coverage among adults was highest among adults ≥ 65 years (60.4%) and lowest among adults 18–49 years (31.8%).
- Adults 18–64 years with high risk conditions had higher coverage 40.8%) than adults 18–64 years without high risk conditions (32.7%).
|
Age Group |
November 2014 |
November 2015 |
|---|---|---|
| All adults (≥ 18 years) |
40.4 ± 1.8 |
39.9 ± 1.9 |
| 18-49 years |
31.4 ± 2.7 |
31.8 ± 2.8 |
| 50-64 years |
43.9 ± 3.2 |
41.3 ± 3.4 |
| 18-64 years |
35.5 ± 2.1 |
34.9 ± 2.2 |
| 18-64 years with high risk conditions|| |
43.2 ± 4.1 |
40.8 ± 4.3 |
| 18-64 years without high risk conditions |
32.6 ± 2.4 |
32.7 ± 2.6 |
| ≥ 65 years |
61.7 ± 3.7 |
60.4 ± 3.9 |
Flu Vaccination Coverage by Race/Ethnicity
- Among non-Hispanic white children, coverage was 5.0 percentage points lower (Table 4) compared to the same time last season.
- For all other racial/ethnic groups, coverage among children was similar compared to coverage at the same time last season.
- There were two early season differences between the racial/ethnic groups:
- Non-Hispanic black (42.6%) and children of non-Hispanic other or multiple races (48.8%) had higher coverage compared to non-Hispanic white children (35.2%).
|
Racial/ethnic Group |
November 2014 |
November 2015 |
|---|---|---|
| Children (6 months-17 years) |
42.0 ± 2.5 |
39.2 ± 2.7 |
| Hispanic |
42.9 ± 6.1 |
42.1 ± 6.7 |
| Non-Hispanic, white only |
40.2 ± 2.7 |
35.2 ± 3.1§‡‡ |
| Non-Hispanic, black only |
46.3 ± 8.8 |
42.6 ± 6.7‡‡ |
| Non-Hispanic, other or multiple race |
42.6 ± 7.1 |
48.8 ± 10.4‡‡ |
- For all racial/ethnic groups, coverage among adults was similar compared to the same time last season (Table 5).
- Among adults, there was only one early season difference between the racial/ethnic groups.
- Non-Hispanic white adults had higher coverage (41.6%) compared to non-Hispanic black adults (35.5%).
|
Racial/ethnic Group |
November 2014 |
November 2015 |
|---|---|---|
| Adults (≥ 18 years) |
40.4 ± 1.8 |
39.9 ± 1.9 |
| Hispanic |
36.5 ± 5.2 |
36.8 ± 5.9 |
| Non-Hispanic, white only |
41/3 ± 2.3 |
41.6 ± 2.3‡‡ |
| Non-Hispanic, black only |
39.2 ± 4.6 |
35.5 ± 5.3‡‡ |
| Non-Hispanic, other or multiple race |
42.7 ± 6.2 |
37.9 ± 6.5 |
Place of Vaccination
- The most common place of vaccination among both adults and children early in the 2015–16 season was a doctor’s office (children: 63.7%; adults: 33.0%). Other medical places included hospital or emergency department (children: 3.7%; adults 6.6%) or clinic, health center, or other medical place (children: 19.0%; adults: 8.3%) (Figure 2).
- Among children, the most common non-medical places of flu vaccination were school (6.2%) and pharmacy (3.2%).
- Other common places of flu vaccination reported by adults included pharmacy (24.8%) and workplace (18.1%).
- These results are similar to estimates from the early 2014–15 season; early in that season 63.3% of children and 33.2% of adults were vaccinated in a doctor’s office.
Figure 2.

What Can Be Done? (Recommendations)
More than half of the United States population 6 months and older had not received a flu vaccination by the end of the survey period. Continued efforts are needed to expand flu vaccination coverage during the next few months of this season to increase the number of people protected against the flu and to reduce the risk of flu, including:
Targeted efforts to eliminate racial and ethnic disparities among adults:
- Differences by race/ethnicity were observed in flu vaccination coverage for this early season. Though coverage among Hispanics was similar to non-Hispanic whites for this early season, disparities in coverage among non-Hispanic blacks were observed. Non-Hispanic black adults had lower flu vaccination coverage than non-Hispanic white adults for this early season. Therefore, continued efforts to increase vaccination coverage among adults in all racial and ethnic groups are necessary to eliminate racial/ethnic differences in flu vaccination coverage. Activities may include:
- Working with leaders in communities with low vaccination coverage to promote vaccination and ensure that all members have access to flu vaccination.
- Working with vaccination providers in these communities to encourage them to routinely assess their patients’ need for flu vaccination at every clinical encounter and offer flu vaccination to all of their unvaccinated patients.
- Working with community leaders and vaccination providers in such communities to create awareness that preventive services like flu vaccination are available without any cost to those who have any kind of insurance.
Implementation of proven strategies to increase vaccination coverage:
- Increased effort is needed to implement strategies proven to increase flu vaccination coverage. Strategies include:
- Health care providers routinely assessing and strongly recommending and offering flu vaccination. Patients are much more likely to get vaccinated when health care providers give a strong recommendation for vaccination.
- The National Vaccine Advisory Committee (NVAC) published the revised Standards for Adult Immunization Practice in 2014. The Standards can be used by all providers to ensure patients are assessed for flu vaccination status at every visit, providers strongly recommend a flu vaccination if needed, a vaccination is provided or the patient is referred for vaccination, and the vaccination is documented.
- Health care providers can utilize Immunization Information Systems, provider assessment and feedback, provider reminders, and standing orders, as well combinations of these interventions, which are evidence-based provider/system strategies to increase vaccination.
- Providers should refer to The Guide to Community Preventive Servicesexternal icon which provides guidance on effective interventions for increasing vaccinationexternal icon.
- Health care providers routinely assessing and strongly recommending and offering flu vaccination. Patients are much more likely to get vaccinated when health care providers give a strong recommendation for vaccination.
Data Sources and Methods
The 2015–16 flu vaccination coverage estimates and findings reported here are early season estimates. These results will differ from final end-of-season coverage estimates expected in September 2016. End-of-season estimates in Figure 1 are from the NIS-Flu for children and the Behavioral Risk Factor Surveillance System (BRFSS) for adults (CDC – Flu Vaccination Coverage, United States, 2014 – 15 Influenza Season and Flu Vaccination Coverage, United States, 2013–14 Influenza Season).
The 2015–16 season estimates in this report are based on two different data sources. Estimates for children are based on data from NIS-Flu, while estimates for adults are based on data from the NIFS. NIS-Flu data from October 1–November 14, 2015 are compared to NIS-Flu data from October 1–November 15, 2014. Adult NIFS data from October 29–November 11, 2015 were compared to NIFS data from October 29–November 12, 2014 (National Early Season Flu Vaccination Coverage, United States, November 2014).
National Immunization Survey-Flu (NIS-Flu)
The NIS-Flu is an ongoing, national list-assisted random-digit-dialed dual frame land line and cellular telephone survey of households with children. It includes three components: the NIS for children 19–35 months, the NIS-Teen for children 13–17 years and a short flu module for all other children 6–18 months and 3–12 years not eligible for the NIS and NIS-Teen identified during the household screening process. Respondents 18 years or older were asked if their child had received a flu vaccination since July 1, 2015 and, if so, in which month and year. The survey interviewers conduct the survey in both English and Spanish; interviews conducted in other languages used language line interpretation services.
Flu vaccination coverage estimates presented in this report are based on interviews conducted from October 1–November 14, 2015. A total of 22,792 NIS-Flu interviews were completed for children 6 months to 17 years. Of these, 5,396 were by landline telephone and 17,396 were by cellular telephone. For reporting place of vaccination, three weeks of NIS interviews (October 25–November 14, 2015) were combined; the place of vaccination estimates are based on 3,888 vaccinated children.
Flu vaccination coverage estimates represent approximately the cumulative proportion of persons vaccinated as of November 14, 2015. Coverage was calculated using an enhanced estimation strategy that resembles the Kaplan-Meier estimation procedure (5). The flu vaccination coverage estimates represent receipt of at least one dose of flu vaccine. Place of vaccination was estimated using simple weighted proportions. All estimates were weighted based on the probability of selection of the telephone number, including adjustments for non-response at the telephone number resolution and household screening stages, probability of selecting the child of interest within the household, and for person non-response. The data were also weighted using a ratio adjustment to population controls (age, sex, race/ethnicity, and geographic area). All NIS-Flu estimates reported here were calculated by NORC at the University of Chicago, utilizing weights they developed.
National Internet Flu Survey (NIFS)
The adult estimates are based on data from the 2015 NIFS, which was conducted by RTI International and GfK Custom Research, LLC and sponsored by CDC, to rapidly collect flu vaccination-related data early during the 2015–16 flu season. The survey was conducted using a probability-based Internet panel designed to be representative of the non-institutionalized U.S. population 18 years or older. The Internet panel survey was conducted in English only.
The sample was stratified by age group and by race/ethnicity. For this ongoing panel, participants are initially chosen by a random selection of telephone numbers and residential addresses. Persons in selected households are then invited by telephone or mail to participate in the web-enabled KnowledgePanel®. For those who agree to participate but do not already have Internet access, GfK provides both a laptop and Internet access at no cost. People who already have computers and Internet service participate using their own equipment. Panelists receive unique login information for accessing surveys online, and are sent e-mails throughout each month inviting them to participate in surveys. The field period of data collection for the NIFS was October 29–November 11, 2015. A survey invitation was sent to a sample consisting of 6,148 panel members. A total of 3,301 completed the NIFS. All NIFS estimates reported here were calculated by RTI, utilizing analysis weights developed by GfK. Flu vaccination coverage estimates represent approximately the cumulative proportion of persons vaccinated as of October 31, 2015. Survey responses “don’t know” and “refused” were excluded from the analyses.
Additional Methods
Differences between groups and between 2014–15 and 2015–16 seasons were determined using t-tests with significance at p < 0.05 and assuming large degrees of freedom (thus using the value of 1.96 for the critical value). Any differences noted as increases or decreases were statistically significant differences; when it is stated that estimates were similar or there was no difference, this indicates that any differences were not statistically significant.
To produce a national estimate of flu vaccination coverage for all persons 6 months and older, the estimates from the NIS-Flu for children and from the NIFS for adults were combined by weighting them by population size (based on census population counts).
Limitations
- The findings reported here are early season estimates and final end-of-season coverage estimates will likely increase.
- Children 6 months–8 years may require two doses of flu vaccine to optimize immunity (3); estimates in this report reflect parental report of at least one dose, and not whether those children requiring two doses were fully immunized.
- NIS-Flu is a telephone survey that excludes households with no telephone service. Non-coverage and non-response bias may remain after weighting adjustments.
- The adult estimates in this report are based on NIFS, an Internet panel survey. Although the Internet panel was probability-based, the estimates may not represent all adults in the United States, and bias may remain after the weighting adjustments.
- All data rely on self-report and are not validated with medical records; validity studies have shown that parental report (for children) and self-report (for adults) may overestimate flu vaccination coverage.
Authors:
Anup Srivastav1, Walter W. Williams2, Tammy A. Santibanez2, Katherine E. Kahn1, Yusheng Zhai1, Peng-Jun Lu2, Carolyn B. Bridges2, Amy Parker-Fiebelkorn2, M. Christopher Stringer3, Jill A. Dever3, Michael G. Bostwick3, Michael S.S. Lawrence4, Mansour Fahimi4, Lin Liu5
1Leidos Inc.
2Immunization Services Division, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention
3RTI International
4GfK Customs Research
5NORC at University of Chicago
Related Links
- FluVaxView Influenza Vaccination Coverage
- Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP) – United States, 2015–16 Influenza Season
- Standards for Adult Immunization Practice
- Flu Vaccination Coverage, United States, 2014-15 Influenza Season
- National Early Season Flu Vaccination Coverage, United States, November 2014
- Flu Vaccination Coverage, United States, 2013-14 Influenza Season
- National Early Season Flu Vaccination Coverage, United States, November 2013
- Flu Vaccination Coverage, United States, 2012-13 Influenza Season
- National Early Season Flu Vaccination Coverage, United States, 2012-13 Flu Season
- Estimated Influenza Illnesses and Hospitalizations Averted by Vaccination — United States, 2013–14 Influenza Season
- Estimated Influenza Illnesses and Hospitalizations Averted by Influenza Vaccination — United States, 2012–13 Influenza Season
- Flu Vaccination Coverage, United States, 2011-12 Influenza Season
- March Flu Vaccination Coverage, National Immunization Survey and National Flu Survey, March 2012
- Results from the November 2011 National Flu Survey – United States, 2011–12 Influenza Season
- National Immunization Survey
- CDC Influenza awareness campaign media relations toolkit, 2013 pdf icon[488 KB, 23 pages]
- Follow CDC Flu on Twitter: @CDCFlu
References
- CDC. Estimates of deaths associated with seasonal influenza–United States, 1976–2007. MMWR 2010;59:1057-1062.
- CDC. Estimated influenza illnesses and hospitalizations averted by vaccination – United States, 2013–14 influenza season. MMWR 2014;63(49):1151-1154.
- CDC. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP) – United States, 2013–2014. MMWR 2013;62(RR07):1-43.
- CDC. Standards for adult Immunization Practice. Available at: https://www.cdc.gov/vaccines/hcp/adults/for-practice/standards/index.html
- Ganesh N, Copeland KR, Davis ND, Singleton JA, Santibanez TA. Modeling H1N1 vaccination rates. Proc JSM Section on Survey Research Methods 2010;5263-5277.
Footnotes
* End-of-season estimates are from the National Immunization Survey-Flu for children (6 months to 17 years) and the Behavioral Risk Factor Surveillance System for adults (18 years or older) (Flu Vaccination Coverage, United States, 2014–15 Influenza Season and Flu Vaccination Coverage, United States, 2013–14 Influenza Season). The 2015–16 end-of-season estimates will not be available until September 2016.
† All percentages in the table are weighted to the U.S. population.
‡ CI=Confidence interval half-width.
§ Statistically significant difference between the 2015–16 season and the 2014–15 season by t-test (p < 0.05).
|| Adults were considered having a high risk condition if they had ever been told by a doctor or other health professional that they had chronic asthma, a lung condition other than asthma, diabetes, heart disease (other than high blood pressure, heart murmur, or mitral valve prolapse), a kidney condition, a liver condition, obesity, sickle cell anemia or other anemia, a neurologic or neuromuscular condition that makes it difficult to cough, or a weakened immune system caused by chronic illness or by medicines taken for chronic illness such as cancer, chemotherapy, HIV/AIDS, steroids, and transplant medicines.
¶ Race-ethnicity is either reported by parent/guardian (NIS-Flu) or self-reported (NIFS). Persons of Hispanic ethnicity may be of any race. Non-Hispanic, other or multiple race includes Asian, American Indian/Alaska Native, Native Hawaiian or other Pacific Islander, multiracial, and other races.
** Pharmacy/Store includes pharmacy or drugstore and local supermarket or grocery store.
†† Other place includes military-related place, other school such as trade school, home, and other unspecified non-medical place.
‡‡ Statistically significant difference for racial/ethnic pair-wise comparisons for the 2015–16 season by t-test (p < 0.05). Among children, non-Hispanic black children and children of non-Hispanic other or multiple races had significantly higher flu vaccination coverage than non-Hispanic white children. Among adults, non-Hispanic black adults had significantly lower coverage than non-Hispanic white adults.
§§ Percentage may not add to 100 due to rounding.